Monocytes & Macrophages . Cirrhosis . Liver failure . TAM Receptors . M-MDSC
Translational Hepatology
Molecular mechanisms of immuneparesis in patients with cirrhosis
Cirrhosis of the liver is a systemic inflammatory condition depicted by its high morbidity and mortality and raising prevalence worldwide. There is no treatment option other than transplantation, applicable to only a minority of patients. Infectious complications are highly frequent and independent predictors of adverse prognosis – being the leading cause of acute decompensation, “acute-on-chronic” liver failure (ACLF) and death. The distinct infection susceptibility in patients with cirrhosis has been attributed to a state termed immuneparesis defined by attenuated immune responses to microbial challenge. A detailed understanding of the mechanisms underlying immuneparesis is desired in order to identify prognostic markers and define potential future immunotherapeutic targets that may enhance immune responses and reduce recurrent infection, need for liver transplantation and death.
Our research group seeks to decipher the pathophysiology of immuneparesis in relation to monocyte and macrophage differentiation and function in patients with cirrhosis. Over the previous years we identified specific immune-suppressive and immune-regulatory monocytic subsets accumulating in the systemic circulation along with disease progression of cirrhosis where they attenuated responses to microbial challenge.
Immune suppression by monocytic myeloid-derived suppressor cells (M-MDSC)
In association with infectious morbidity and mortality reduced expression of the MHC class II receptor human leucocyte antigen (HLA)-DR on circulating monocytes from patients with advanced cirrhosis had been observed a decade ago. The mechanism underlying infection susceptibility remained indeterminate. We recently described that expression of HLA-DR on circulating monocytic cells gradually decreased while severity of cirrhosis increased, and was attributed to the generation of M-MDSC (CD14+CD15−CD11b+HLA-DR−). Functionally, circulating M-MDSCs from patients with cirrhosis ex vivo were typified by distinct immunosuppressive properties, i.e. reduced T cell activation, TNF-α and IL-6 production in response to toll-like receptor (TLR) stimulation and phagocytic capacity. M-MDSC accumulated in response to systemic inflammatory responses (SIRS) and circulating pathogen-associated molecular patterns (PAMPs). In vitro the immune stimulant poly(I:C), reduced abundance of suppressive M-MDSC and augmented their antimicrobial function.
Immune regulation by TAM receptors
Also, we specifically focussed on the regulatory function of tyrosine kinases of the TAM receptor family (Tyro-3, AXL and MERTK). TAM receptors are expressed on monocytes and macrophages and play a pivotal role in regulating innate immune responses to microbial challenge by inhibiting TLR signalling and immune homeostasis by promoting efferocytosis, i.e. phagocytosis of apoptotic cells. We have recently discovered the expansion of circulating immune-regulatory AXL- and MERTK-expressing monocyte subsets in patients with cirrhosis at different stages of disease that were characterised by preserved phagocytosis of bacteria, enhanced efferocytosis but suppressed cytokine responses (TNF-α and IL-6) to lipopolysaccharide and attenuated T cell activation. AXL expressing cells accumulated in response to phagocytosis of bacteria, efferocytosis and PAMP exposure. MERTK- and AXL- inhibition, respectively, restored cytokine responses in vitro.
In the circulation of patients with advanced stages of cirrhosis these described dysfunctional monocytic cell populations prevailed over their functional counterparts and explain reduced capacity to repel microbial challenge and infection susceptibility. Since proof of principle experiments revealed that these immune functions were modifiable, we further investigate whether targeted immune modulatory therapies may restore innate immune responses of monocytes from patients with cirrhosis in the future. Importantly, our observations also indicate that these cells evolve in a highly compartment specific manner, and initiated our current and ongoing project entitled “Diversity and compartmentalisation of monocytes & macrophages and immuneparesis in patients with cirrhosis”.
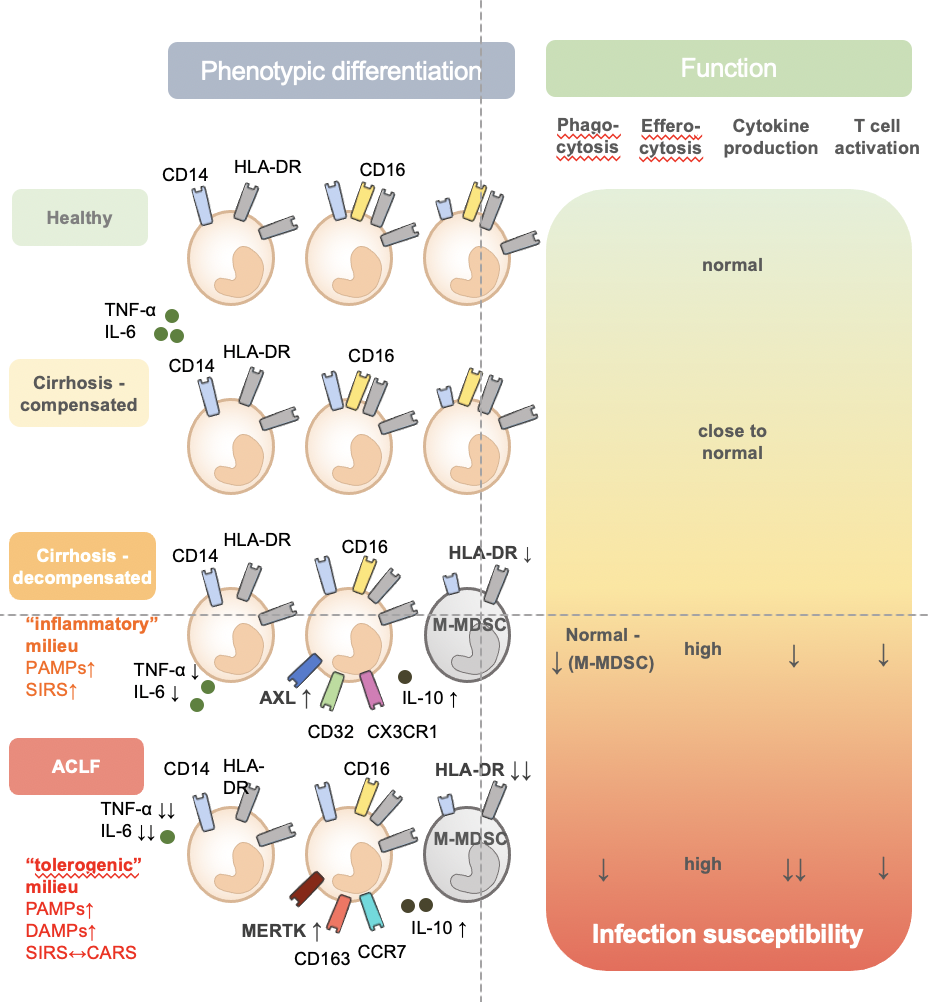
Differentiation of circulating monocytic cells along with disease severity of cirrhosis. Classically monocytes have been subdivided into CD14++CD16- (classical), CD14++CD16+ (intermediate), and CD14+CD16++ (non-classical) subsets. Paralleling progression of cirrhosis towards decompensation and acute-on-chronic liver failure (ACLF), distinct immune-regulatory and immune-suppressive monocytic subsets accumulate and displace functionally intact monocytic cells and hereby may relate to increased infection susceptibility. Immune-suppressive monocytic myeloid-derived suppressor cells (M-MDSC) expanded during progression to decompensated stages and represented half of all circulating CD14+ cells in ACLF. During decompensation distinct stage-specific immune-regulatory subsets expanded such as CD14++CD16+, CD14+CD16highHLA-DRhighAXL+ in a predominantly inflammatory milieu, and CD14+CD16highHLA-DRhighCD163+MERTK+ in a predominantly tolerogenic milieu such as ACLF. Adapted from Bernsmeier et al., J Hepatol, 2020. PAMP, Pathogen-associated molecular pattern. DAMP, Damage-associated molecular pattern. SIRS, systemic inflammatory response. CARS, compensatory anti-inflammatory response syndrome.